First published 13/02/2013 at http://grahamdavey.blogspot.co.uk
As promised, it's my intention to post some new pieces written for the second edition of my Psychopathology textbook (due to be published late 2013). This post begins that process with a new section written to introduce and evaluate DSM-5 from the Chapter on Classification & Assessment in Clinical Psychology.
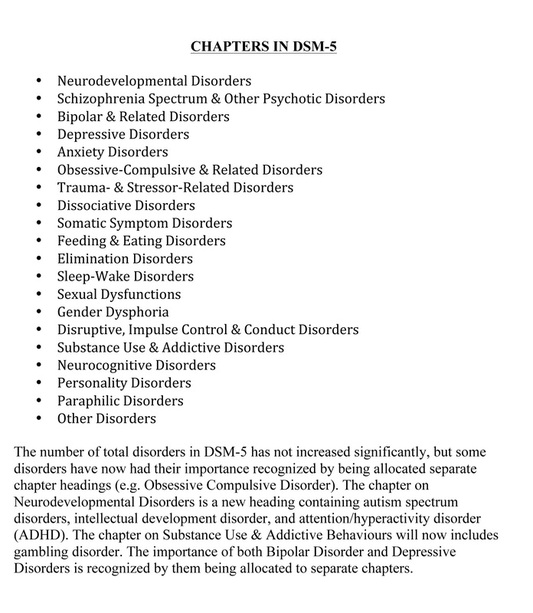
"Published in 2013, DSM-5 arguably represents the most comprehensive revision of the DSM so far, and it has involved many years of deliberation and field trials to determine what changes to mental health classification and diagnosis are essential and empirically justifiable (Main chapter headings for DSM-5 are provided in Table 1).
"Published in 2013, DSM-5 arguably represents the most comprehensive revision of the DSM so far, and it has involved many years of deliberation and field trials to determine what changes to mental health classification and diagnosis are essential and empirically justifiable (Main chapter headings for DSM-5 are provided in Table 1).
The main changes between DSM-5 and its predecessor (DSM-IV-TR) are listed in Table 2.
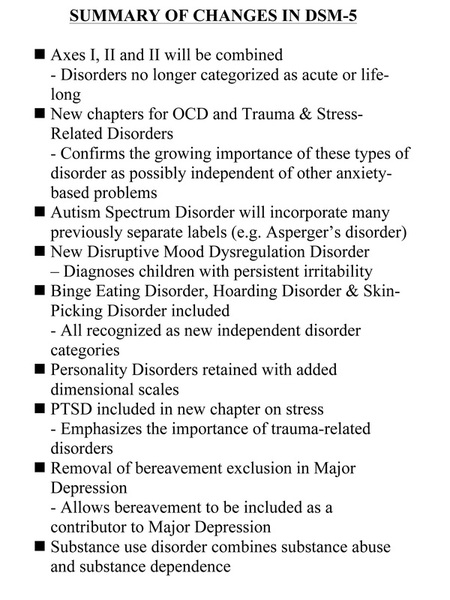
First, previous versions of DSM placed mental health problems on a number of different axes representing clinical disorders (Axis I), developmental and personality disorders (Axis II), or general medical conditions (Axes III). This multiaxial system has been scrapped – largely because there was not enough evidence to justify the differences between them. Instead, in DSM-5 clinicians will be encouraged to rate severity of symptoms along continuums developed for each disorder. Secondly, the importance of some disorder categories has been recognised either by allocating them to their own chapter or by recognising them as new individual diagnostic categories. For example, Obsessive-Compulsive Disorder (OCD) is recognized as a significant mental health problem by being allocated it’s own chapter in DSM-5, and new diagnostic categories within this chapter include Hoarding Disorder (see Chapter 6) and Excoriation Disorder (skin-picking disorder). Similarly, DSM-5 has a new chapter on Trauma & Stress-Related Disorders that now includes Post-Traumatic Stress Disorder (PTSD). DSM-5 focuses more on the behavioural symptoms that accompany PTSD and proposes four distinct diagnostic clusters instead of the previous three. Thirdly, major changes have been made to the criteria for diagnosing Autism Spectrum Disorder (ASD), Personality Disorders, Specific Learning Disorders, and Substance Use Disorders. Autistic Spectrum Disorder has become a diagnostic label that will incorporate many previous separate labels (e.g. Asperger’s disorder, childhood disintegrative disorder, pervasive developmental disorder) in an attempt to provide more consistent and accurate diagnosis for children with autism (see Chapter 16). DSM-5 will retain the categorical model for Personality Disorders outlined in DSM-IV-TR, but rating scales are provided to assess how well an individual’s symptoms fit within these different types (Chapter 12). The new Specific Learning Disorder category is broadened to represent distinct disorders which interfere with the acquisition and use of one or more of a number of academic skills, including oral language, reading, written language or mathematics (Chapter 15), and the new Substance Use Disorder category will combine the previous DSM-IV-TR categories of substance abuse and substance dependence into one overarching disorder. Some other important changes include (1) the elevation of Binge Eating Disorder from an appendix to a recognized diagnostic category, (2) Disruptive Mood Regulation Disorder as a new category for diagnosing children who exhibit persistent irritability and behavioural outbursts, and (3) the removal of the “bereavement exclusion” from the diagnosis of Major Depression; this means that depressive symptoms lasting less than two months following the death of a loved one can be included amongst the criteria for diagnosing Major Depression, and reflects the recognition that bereavement is a severe psychological stressor that can precipitate major depression.
Criticisms of Changes in DSM-5: While these most recent changes to the DSM have been extensively discussed and researched, many of the revisions have been received critically, and it is worth discussing some of these criticisms because they provide an insight into the difficulties of developing a mental disorders classification system that is fair and objective.
First, many of the diagnostic changes will reduce the number of criteria necessary to establish a diagnosis. This is the case with Attenuated Psychosis Syndrome, Major Depression, and Generalized Anxiety Disorder, and this runs the risk of increasing the number of people that are likely to be diagnosed with common mental health problems such as anxiety and depression. It is a debatable point whether increases in the number of diagnosed cases is a good or a bad thing, but it is likely to have the effects of “medicalizing” many everyday emotional experiences (such as ‘grief’ following a bereavement, or worry following a stress life event), and creating “false-positive” epidemics (Frances, 2010).
Secondly, DSM-5 has introduced disorder categories that are designed to identify populations that are at risk for future mental health problems, and these include Mild Neurocognitive Disorder (which would diagnose cognitive decline in the elderly) and Attenuated Psychosis Syndrome (seen as a potential precursor to psychotic episodes). Once again, these initiatives run the risk of medicalizing states that are not yet full-blown disorders, and could facilitate the diagnosis of normal developmental processes as psychological disorders.
Thirdly, there are concerns that changes in diagnostic criteria will result in lowered rates of diagnosis for some particularly vulnerable populations. For example, applying the DSM-5 criteria for Autism Spectrum Disorder to samples of children with DSM-IV-TR diagnoses that would no longer be available in DSM-5 suggested that 9% of this latter group would lose their autism diagnosis with the introduction of the new DSM-5 criteria (Huerta, Bishop, Duncan, Hus & Lord, 2012). Similar concerns have been voiced about changes to Specific Learning Disorder diagnostic criteria in DSM-5, and the possibility that deletion of the term dyslexia as a diagnostic label will disadvantage individual with specific phonologically-based, developmental reading disabilities (http://www.disabilityrightsohio.org/news/dsm5-dyslexia-june-2012).
Finally, two enduring criticisms of DSM generally that have continued to be fired specifically at DSM-5 have been that (1) DSM-5 has continued the process of attempting to align it’s diagnostic criteria with developments and knowledge from neuroscience (Regier, Narrow, Kuhl & Kupfer, 2011), when there is in fact very little new evidence from neuroscience that helps define specific mental health problems, and (2) most mental health problems (and psychological distress generally) are now viewed as dimensional, so any criteria defining a diagnostic cut-off point will be entirely arbitrary. DSM-5 has attempted to recognise the importance of the dimensionality of symptoms by introducing dimensional severity rating scales for individual disorders. But as we have seen from the discussion above, each iteration change in DSM diagnostic criteria changes the number and range of people who will receive a diagnosis, and this makes it increasingly hard to accept diagnostic categories as valid constructs (e.g. Kendler, Kupfer, Narrow, Phillips & Fawcett, 2009).
Despite its conceptual difficulties and its many critics, DSM is still the most widely adopted classification and diagnostic system for mental health problems. Such a system is needed for a number of reasons, including determining the allocation of resources and support for mental health problems, for circumstances that require a legal definition of mental health problems, and to provide a common language that allows the world to share and compare data on mental health problems. Having said this, there are still many significant problems associated with DSM, and diagnosing and labelling people with specific psychological disorders raises other issues to do with stigma and discrimination. Indeed, we should be clear that diagnostic systems are not a necessary requirement for helping people with mental health problems to recover, and many clinical psychologists prefer not to use diagnostic systems such as DSM-5, but instead prefer to treat each client as someone with a unique mental health problem that can best be described and treated using other means such as case formulation (see Section 2.3 for a fuller description and examples of case formulation)."
Criticisms of Changes in DSM-5: While these most recent changes to the DSM have been extensively discussed and researched, many of the revisions have been received critically, and it is worth discussing some of these criticisms because they provide an insight into the difficulties of developing a mental disorders classification system that is fair and objective.
First, many of the diagnostic changes will reduce the number of criteria necessary to establish a diagnosis. This is the case with Attenuated Psychosis Syndrome, Major Depression, and Generalized Anxiety Disorder, and this runs the risk of increasing the number of people that are likely to be diagnosed with common mental health problems such as anxiety and depression. It is a debatable point whether increases in the number of diagnosed cases is a good or a bad thing, but it is likely to have the effects of “medicalizing” many everyday emotional experiences (such as ‘grief’ following a bereavement, or worry following a stress life event), and creating “false-positive” epidemics (Frances, 2010).
Secondly, DSM-5 has introduced disorder categories that are designed to identify populations that are at risk for future mental health problems, and these include Mild Neurocognitive Disorder (which would diagnose cognitive decline in the elderly) and Attenuated Psychosis Syndrome (seen as a potential precursor to psychotic episodes). Once again, these initiatives run the risk of medicalizing states that are not yet full-blown disorders, and could facilitate the diagnosis of normal developmental processes as psychological disorders.
Thirdly, there are concerns that changes in diagnostic criteria will result in lowered rates of diagnosis for some particularly vulnerable populations. For example, applying the DSM-5 criteria for Autism Spectrum Disorder to samples of children with DSM-IV-TR diagnoses that would no longer be available in DSM-5 suggested that 9% of this latter group would lose their autism diagnosis with the introduction of the new DSM-5 criteria (Huerta, Bishop, Duncan, Hus & Lord, 2012). Similar concerns have been voiced about changes to Specific Learning Disorder diagnostic criteria in DSM-5, and the possibility that deletion of the term dyslexia as a diagnostic label will disadvantage individual with specific phonologically-based, developmental reading disabilities (http://www.disabilityrightsohio.org/news/dsm5-dyslexia-june-2012).
Finally, two enduring criticisms of DSM generally that have continued to be fired specifically at DSM-5 have been that (1) DSM-5 has continued the process of attempting to align it’s diagnostic criteria with developments and knowledge from neuroscience (Regier, Narrow, Kuhl & Kupfer, 2011), when there is in fact very little new evidence from neuroscience that helps define specific mental health problems, and (2) most mental health problems (and psychological distress generally) are now viewed as dimensional, so any criteria defining a diagnostic cut-off point will be entirely arbitrary. DSM-5 has attempted to recognise the importance of the dimensionality of symptoms by introducing dimensional severity rating scales for individual disorders. But as we have seen from the discussion above, each iteration change in DSM diagnostic criteria changes the number and range of people who will receive a diagnosis, and this makes it increasingly hard to accept diagnostic categories as valid constructs (e.g. Kendler, Kupfer, Narrow, Phillips & Fawcett, 2009).
Despite its conceptual difficulties and its many critics, DSM is still the most widely adopted classification and diagnostic system for mental health problems. Such a system is needed for a number of reasons, including determining the allocation of resources and support for mental health problems, for circumstances that require a legal definition of mental health problems, and to provide a common language that allows the world to share and compare data on mental health problems. Having said this, there are still many significant problems associated with DSM, and diagnosing and labelling people with specific psychological disorders raises other issues to do with stigma and discrimination. Indeed, we should be clear that diagnostic systems are not a necessary requirement for helping people with mental health problems to recover, and many clinical psychologists prefer not to use diagnostic systems such as DSM-5, but instead prefer to treat each client as someone with a unique mental health problem that can best be described and treated using other means such as case formulation (see Section 2.3 for a fuller description and examples of case formulation)."
 RSS Feed
RSS Feed